
October 2023
By: Chris Beebe, SVP, Compliance & Regulatory Services at CPS
My team and I visit lots of hospital pharmacies, both those we manage and those with which we consult. We’re getting the most questions (and confusion) when we talk about the competencies required in revised USP Chapter <797>.
Here're some more questions and answers that might help you.
First: Let's make the complicated easier to understand.
I recently talked about the supply expense and incubation logistics related to all the new touch media that would be needed under the revisions, including plates and paddles. Things are going to get more complicated than you think.
For example: Under the revised standards, we'll now test our compounders twice as often. That means you can expect your touch media supply utilization to double, right? Wrong. It will actually be quintupled.
It all comes down to this: USP's new competency format is more complex. Rather than two plates or paddles per year, compounders will soon need to use 10.
Here's another example:
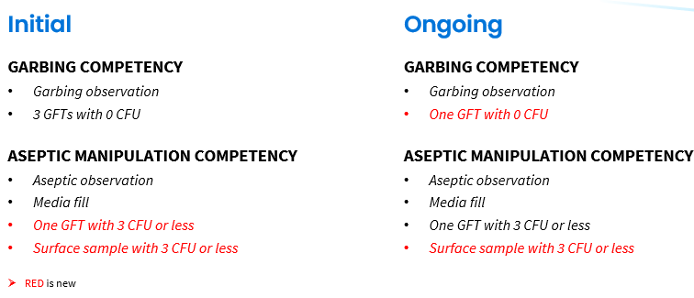
We’re all aware of the initial competencies requiring gloved fingertip testing (GFTs), right...three times after garbing when a new compounder comes on board. It has to have zero CFU, right? No growth at all. That’s because it’s intended to see if the compounders can keep their gloves totally clean during the garbing and hand hygiene process.
Here's what's new:In the ongoing testing required by the revised chapter, we’ll now also do one GFT after garbing with zero CFU. Then we’ll do the media fill, then we’ll do a second GFT with < 3 CFU to pass. We’re used to this one. But what’s the difference?
The post-media fill GFT is designed to help us assess how clean we can keep our gloves while compounding. Touching things may lead to growths, which is why some CFU are allowed. It just can’t be too much.
And finally...
There’s the new surface sample at the end of it all, to see how well we can minimize contamination of the compounding deck. All these extra steps are more of an issue for the tester, not the person being tested.
Here’s your takeaway: I’ve been encouraging our hospital partners and peers to do some practice sessions to see how long it takes and get the testers used to the flow. You, too, can heed this advice.
Here's what it can look like: You’ll have five plates or paddles to juggle now, and each of those will need to be properly labeled with both the hand (left or right) and the CFU threshold (zero or three). All this while garbed and keeping the area clean too!
This visual may help you get started.
As you can see, some rehearsals will go a long way to get you and your team ready before you actually start. I’d be happy to talk through strategies with you and discuss some of the successes I’ve seen at our CPS sites. Connect with me on LinkedIn or drop me an email: chris.beebe@cps.com.
Read More: USP <797>: The Most Challenging Revisions: Part 1
 Follow us on Linkedin
Follow us on Linkedin